


The Disregard of Mask Wearing
With apologies to Bonham and their 1989 album, The Disregard of Time Keeping

During the leadup to the holidays, the CDC and various state, local, and hospital officials again asked that people wear masks in public / indoors to address the current tripledemic of COVID, flu, and RSV (not to mention other infections also on the rise that we’re potentially more vulnerable to as a result of a COVID infection). At the same time, we continue to see pieces like The Last Holdouts and The Case for Wearing Masks Forever, that even if not their intent, still manage to reinforce perceptions that the pandemic is over for most of us, individual risk is really all that matters, risk mitigation is only all or nothing instead of a layered approach adaptive to local conditions, and that anyone still masking is an overly fearful person who should be pitied, or worse, bullied. I recommend reading Dr. Gregg Gonsalves’s recent thoughtful critique of The Last Holdouts.
But in reality, the pandemic isn’t over. Thanks to our own ongoing collective behavior (inadequate monitoring of transmission, inadequate vaccination, inadequate ventilation/filtration, inadequate mask wearing when needed, etc.) the virus is still easily spreading. Health risks from the initial infection itself, as well as Long COVID (about which we still have much to learn), are still with us, though worse for the immunocompromised, the elderly, and others with certain pre-existing health conditions. Negative impacts to our healthcare and public education systems continue, as do the impacts to our workforces and the economy at large. These negative impacts also continue to be inequitably distributed, and the ongoing transmission increases the likelihood of worse variants evolving. The current high transmission rates in China should be particularly concerning relative to viral evolution (on top of the obvious humanitarian disaster).
So while masks themselves, given the right material, can be highly effective at capturing viral containing aerosols from the air, associated behavioral factors can limit that effectiveness. Such behavioral factors range from keeping a mask sealed properly on your face to politicizing the act of mask wearing itself. These behavioral factors are one reason why mask wearing, and personal protective equipment (PPE) in general, are listed at the bottom of the hierarchy of hazard controls inverted pyramid below (the ease of damage of such PPE is another reason).

{kind=link}
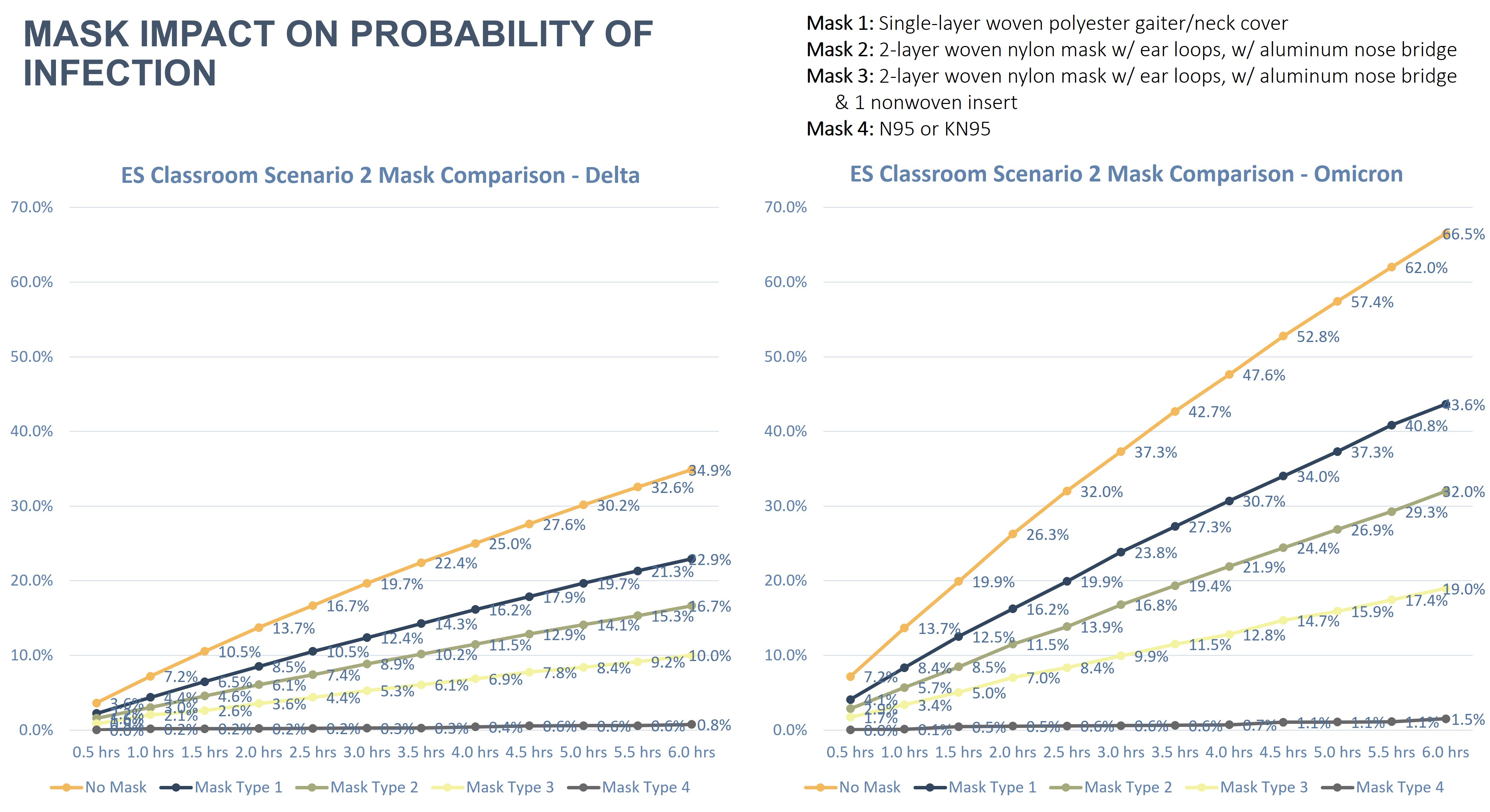
But due to the comparative ease and speed with which masks can be deployed compared to the implementation of other strategies at higher levels within the hierarchy (e.g., upgrading a building’s HVAC system), we should expend more effort to understand and address the behavioral/social barriers to effective mask wearing. We can’t really afford to disregard it as a strategy. As is apparent from the figure below, the importance of mask wearing, and increasing mask efficiencies, to our health indoors increases as variant infectiousness increases (comparing Delta to Omicron in this particular example). This is true even when accounting for vaccinations, typical non-hospital ventilation and mechanical system filtration levels, and the addition of portable air cleaners.
Mask wearing, by reducing viral transmission among our various workforces, also increases the “health” of our businesses and larger economy. In an August 2022 article from the Brookings Institute, it was estimated then that as many as 4 million workers were likely out of work as a result of long COVID, translating to $230 billion in lost U.S. earnings or nearly 1.4% of the total U.S. gross domestic product. If we also include the economic burden associated with the lower productivity of people working while ill, the associated patient healthcare costs, and the lost productivity of caretakers, that number rises to $544 billion. And if those with long COVID don’t start recovering at faster rates (and/or we don’t do a better job of limiting transmission), these numbers will only grow.
To see how this can play out at an organizational level, during the summer of 2022 we provided retrocommissioning services to a Federal client looking to improve their building’s energy efficiency and employee’s health and wellness. Part of that effort included estimating the health and productivity impacts from the various proposed building and operational improvements (including mask wearing). We modeled the annual productivity losses resulting from being out sick with COVID and for a smaller percentage of employees contracting long COVID. We did this for the existing conditions and each of the proposed packages of improvements. For each of those models, we compared 0% employee mask wearing to 100% employee mask wearing (using an N95 respirator).
One hundred percent mask wearing resulted in an estimated reduction of annual lost productivity ranging from $276,000 to $528,000, depending on the building condition (existing vs proposed improvements). For context that’s about 1% to 1.8% of the organizations total annual payroll. It’s also a conservative estimate, assuming a) only 3.25 net working days are lost per infection, b) an employee can only be infected once per year, and c) employees are only exposed to an infected person 2.5% of their time in the office over the course of a year. Nor does this account for any lost efficiencies from working at home while symptomatic or for the impacts on other employees when co-workers are out sick.
But while plenty of data exists on the collective and individual benefits of mask wearing at reducing the risk of viral transmission – of basically acting as a personal safety device while breathing in viral contaminated air – the ability to remove viral containing aerosols is but one of many determining factors for individual or collective decisions to wear them. Mask functionality isn’t defined solely based on their ability to filter out pollutants. The choice of whether or not to wear anything, how to wear it, and how to decorate it, commonly acts as a cultural signal, symbolic of values, group membership, and other forms of social meaning.
To see that in action, spend some time observing the variety of clothing styles present within a high school. As I’ve written elsewhere, a high schooler’s perspective of acceptable clothing is shaped by peers and family, school policy, and society in general. Clothing is also used as a means of establishing their group identity as well as signaling membership in that group. For teenagers who are still maturing and experimenting with who they eventually want to be and what groups they want to belong to, clothing is part of that experimentation.

Masks are no different. As something highly visible that we adorn our bodies with, the choice of whether or not to wear a mask, the type of mask worn, how it’s being worn, where it’s being worn, along with any symbols, decorations, or patterns emblazoned on the mask, can all encode information and signal meaningful social cues, like social identity.
For some cultural and political affiliations, mask wearing has negative connotations. Research has shown that within the honor cultures of the U.S. South and other areas, during the pandemic masks have become symbols of weakness (both in terms of displaying fear and being overly susceptible to illness), at odds with portraying strength and toughness, and negatively impacting one’s social status and honor. There is significant peer pressure within these groups to not wear masks (somewhat stronger for males), and wearing masks in such contexts can negatively impact their wellbeing through various forms of ostracization. So given this, how could the perception of mask wearing be flipped in these cultures? What could be done to portray the absence of masks when transmission is high as offensive and weak? How could mask wearing (and its promotion) to protect COVID-19’s most vulnerable be portrayed as the honorable thing to do?
Other research has shown, looking at nations, U.S. states, and individuals, that collectivism (“the tendency to be more concerned with the group’s needs, goals, and interests than with individualistic-oriented interests” as well as the view of an interdependent self) is much more strongly associated with mask wearing compared to individualism (“the tendency to be more concerned with one’s own needs, goals, and interests than with group-oriented concerns” as well as the view of an independent self). One way to temporarily create high levels of collectivism even among groups defined by high degrees of individualism, is to have a common external enemy providing an imminent threat. How could we better portray SARS-COV-2 as that common enemy (made more difficult by it being too small to see), and the threat as real and imminent?

Not surprisingly many conservatives associate mask mandates with government overreach and are less likely to view masks as effective, exacerbated by a greater distrust compared to liberals of government and public health officials, and experts in general. Compared to liberals, conservatives are also more likely to associate mask wearing with negative emotional wellbeing (via an infringement on personal liberties, loss of honor, negative impact on public image, and ostracization by one’s community). Liberals are more likely to associate mask wearing with civic duty, tied to a greater trust in government and experts.
Though it should be noted that as the pandemic has progressed, many liberals also increasingly associate mask wearing with negative emotional wellbeing, likely contributed to by increasing societal fatigue with risk mitigation measures. Large scale collective mask wearing to address the seasonal spread of respiratory diseases hasn’t historically been part of the U.S.’s (or many other western nation’s) normative public health response. As it isn’t a cultural norm, fatigue and backlashes are inevitable if this isn’t specifically recognized and addressed, as pointed out by some researchers. And because it’s not the norm, measures like shaming that can be effective in some contexts can actually backfire, further reducing mask wearing. So how do we move toward making this part of our normal, accepted public health response? One that our leaders and public health officials are willing to implement and enforce as needed?
At the individual and small group level, we likely need to expend more effort making the negative outcomes of high transmission rates real to people. They need to see the connections to their own lives, loved ones, and communities, as some research has shown that those who perceive a greater impact of COVID-19 on their day-to-day are more likely to wear masks voluntarily. For a business owner, maybe that’s seeing the projected impacts to their workforce and their own bottom line from a consultant they trust. For others, maybe that’s hearing from an immunocompromised cousin how it impacts their emotional and practical day-to-day, how it increases their isolation. Or hearing from a family member who’s a nurse how this is impacting his daily stress levels, healthcare staffing issues, and the resulting quality of care one might receive in a hospital.
Note the trust and social connections inherent in the above examples. These messages about the real threats of SARS-CoV-2 and the effectiveness of masks to limit transmission (counteracting circulating mask wearing misinformation) need to come from people they trust, from within their own groups, as various research has shown (here’s one example). And any mask wearing mandates or policy, messaging campaign, etc., must take into account the interaction of all of the above factors plus others (like tightness and looseness) relevant to the level and context being focused on - organization, community, state, etc.
It’s also likely that many aspects of individual and collective behavior in addition to what’s been mentioned above need to be addressed at multiple levels of U.S./western society for mask wearing to be a normative public health measure that can be effectively implemented as needed. The extreme levels of hyper-partisanship, the distrust of public officials, government, and scientists/experts, society’s narrow definition of economic value, and the toxic individualism that varyingly plague societies and communities are just some of what need to be addressed.

Another functional aspect of mask wearing requiring further examination is its impact on communication, both verbal and non-verbal. Our faces are intensely communicative, arguably the most expressive parts of our bodies. Our facial muscles and skin operating together can convey a wide range of thoughts, emotions, and other non-verbal cues (nonverbal communication is said to comprise over 50% of our overall communication). Covering half of our face (in addition to muffling our voices) modifies the modes of communication and expression that we consider habitually normal. As a result it can negatively impact our ability to interact with one another in certain contexts, as well as our ability to navigate existing social relationships or build new ones.
However, it’s also true that our brains are fairly adaptable, and it has been argued based on some research that given time, most of us can adapt to communicating while wearing masks, particularly when in familiar contexts and discussing familiar topics. Some research also suggests that wearing masks doesn’t have a negative impact on the early childhood development of speech and social skills. But more research is needed to fully understand the impacts of mask wearing on communication and learning.
Some of this existing research indicates difficulties in communication while wearing a mask may increase when one or more of the people engaged in conversation is unfamiliar with aspects of the conversation’s topic and/or the path taken by the conversation is less predictable. Such situations are likely to increase in cross-cultural contexts, as we know that facial expressions as well as their interpretations can vary culture to culture, exacerbated when those communicating don’t share a common language that all participants are fluent in. And for some deaf and hard of hearing individuals, eliminating lip reading and certain facial expressions from their modes of communication can also makes things more difficult.
Early in the pandemic there was recognition of these negative impacts on communication, with varying efforts made to address them. The image below is from a 2020 article offering some tips for interpreting non-verbal communication with only the upper half of our faces showing (also see the following article). It should be noted that the article doesn’t acknowledge national, cultural or potential other demographic differences in facial expressions and their interpretations. Future guides should consider these factors as well (and there may be some out there I’m unaware of).

In addition to interpretation guides and mask technological innovations (like high efficiency, see-through masks), the impacts on communication can also be minimized by taking into account certain aspects of the built environment. Our facilities could be better optimized to support communication while wearing masks, or at least compensate for any associated frustrations and anxiety generated, to help minimize this particular negative impact.
For examples, it’s certainly important to have adequate levels of good quality, glare-free lighting, particularly in the vertical plane, to aid in interpreting these non-verbal cues. It’s also possible that luminaire color temperature may impact this through one’s formative experiences growing up viewing interactions of warm vs cool color temperatures, daylight color temperatures, specific skin tones, etc., though research would be needed here to verify this and understand the details.
For verbal communication with masks, minimizing background noise levels becomes even more important, given the muffling of voices and the lack of interpretive context provided by lip reading and facial expressions. In a classroom setting, mask wearing makes voice amplification systems that much more critical. And by creating environments that are at least comfortable regarding other aspects of indoor environmental quality (IEQ), that are functional, inviting, etc., we at least minimize additional stresses and distractions that take away from the needed mental and emotional focus/energy for communicating while wearing masks. Note that addressing these communication issues could also be important for improving the acceptance of mask wearing among conservatives (or at least removing a justification for not wearing them), as some research has shown there is a correlation between conservatism and a lower perceived utility for masks.

This post has focused on a few mask functionality issues that likely need to be addressed if mask wearing is to become more of a normative public health measure in the U.S. and other western nations. Beyond functionality, there are three additional issues deserving attention, but I will only briefly mention them as this is already a lengthy post. The first is the negative environmental impacts associated with the lifecycle of disposable masks. The second is the use of slave labor to meet the disposable mask demands of wealthy nations (including the U.S.). And the third is the inequitable access to high efficiency respirators (compounding the inequities found in building ventilation and filtration capabilities as well as facility quality overall). All three really need to be addressed if mask wearing becomes more of a global norm.
Mask wearing can be a highly effective means for reducing the spread of COVID-19 and other respiratory diseases. But to make it more of a normative public health measure within the U.S. - more likely to be implemented by our leaders and public health officials as needed, with greater acceptance by the general public and less subject to fatigue - we need to better understand and address the social/cultural meanings associated with mask wearing and its impact on communication. Otherwise we’ll likely continue to collectively disregard it.